Acknowledgements
This guide was written by Natalie Lovell, Policy Analyst, and Jo Bibby, Director, Healthy Lives Strategy, at the Health Foundation.
Thank you to all the public health experts and others who contributed to this guide.
Introduction
What causes heart disease? To some, the clear answer would be blocked arteries. But what causes those arteries to become blocked? Perhaps it’s the unhealthy food and drink people consume, their lack of exercise, or their stress levels. And what, in turn, makes them feel stressed, shapes their opportunities to be active and determines their choices about what they eat and drink?
The answers lie in the circumstances in which people are born, grow, live, work and age: the social determinants of health (see Box 1). These can enable individuals and societies to flourish, or not. These are the causes of the causes.
The Health Foundation has written this guide as a brief introduction to the social determinants of health. It explains how a person’s opportunity for health is influenced by factors outside the health and social care system. It also shows that many people don’t have the same opportunities to be as healthy as others.
With the help of short case studies, it highlights how action can create improvements in the health of the whole population, for the lasting benefit of individuals, society and the economy.
The guide has been written for anyone with an interest in people’s health and wellbeing. It will be especially useful to those new to the social determinants of health.
Why focus on the social determinants of health?
A person’s opportunity for good health starts long before they need health care., So, there is a compelling case that responsibility for the health of the public should go beyond the health and social care system to span all of society.
A wide range of organisations – across government, the voluntary sector, the private sector, media, advertising and local communities – have it within their power to improve people’s health. By acknowledging and acting on this, it is possible to harness a multitude of opportunities to overcome the big health challenges of today.
Box 1: The factors that influence health and wellbeing – terminology and scope
Throughout this guide we use the term ‘social determinants of health’. These are sometimes also called the wider determinants of health. When we use the term, we are referring to the social, cultural, political, economic, commercial and environmental factors that shape the conditions in which people are born, grow, live, work and age.
The health and social care system is also an important social determinant of health that supports everyone at different points in their lives. However, this guide focuses beyond health and social care to areas where there is untapped potential for local and national action to support healthier lives.
* The term ‘causes of the causes’ refers to the underlying causes of health problems. Find out more: Rose G. Sick individuals and sick populations. International Journal of Epidemiology. 1985;14(1):32–8.
What is ‘health’?
Most people associate the word ‘health’ with hospitals and doctors. When considering ‘good health’ they tend to think simply of an absence of illness. In this guide, we refer to health in its broadest sense: a person’s level of good physical and mental health, and the extent to which individuals in a society are enabled to live healthy and flourishing lives.
This guide describes the factors in the daily lives of people in the UK that create and support health and wellbeing.
Through this lens, a healthy person is someone with the opportunity for meaningful work, secure housing, stable relationships, high self-esteem and healthy behaviours.
A healthy society, in turn, is not one that waits for people to become ill, but one that sees how health is shaped by social, cultural, political, economic, commercial and environmental factors, and takes action on these for current and future generations.
[Health is] not just the physical wellbeing of an individual but also the social, emotional and cultural wellbeing of the whole community, in which each individual is able to achieve their full potential as a human being, thereby bringing about the total wellbeing of their community.
Aboriginal Health and Medical Research Council of New South Wales, Australia
Box 2: Wellbeing
Put simply, wellbeing is ‘about “how we are doing” as individuals, communities and as a nation and how sustainable this is for the future.’
Some people use this term – alongside health or on its own – because it encompasses health but also goes beyond it, helping them capture a more rounded picture of healthy lives.
† This approach to health is loosely based on a model called ‘salutogenesis’, developed by medical sociologist Aaron Antonovsky.
Why is good health important?
Good health is of social and economic value to individuals, society and the economy. It is an enabler of the prosperous and flourishing societies that governments strive to achieve.
Thinking about the value of good health encourages a focus on the benefits of creating health and wellbeing in today’s environments, rather than simply treating disease in individuals. It provides the basis for considering the moral, social and economic case for investing in action that creates and maintains health.
The ultimate source of any society’s wealth is its people. Investing in their health is a wise choice in the best of times, and an urgent necessity in the worst of times.
David Stuckler, The body economic: why austerity kills
The moral case
The moral case for maintaining and improving people’s health has been made from several perspectives, including the following.
- The welfare state – in 1942 Sir William Beveridge published a report making recommendations aimed at tackling unemployment, the cost of childcare, a lack of good housing, and public health issues such as malnutrition. The report was popular and the main political parties agreed that the recommendations would help create a more equal society.
- Good health is a basic human right – it featured in the United Nations’ Universal Declaration of Human Rights (Article 25) in 1948. It is also one of the core principles in the Constitution of the World Health Organization.
- The capability approach – this relates to the moral importance of a person having what they need (for example, good health and a home) to do the things they wish to do and live a good quality of life. The case for this approach was first made by economist and philosopher Amartya Sen in the 1980s. Seen from this perspective, health and wellbeing is a resource for living, and is a matter of social equity and justice.
Today, the UK is a wealthy society. Yet a baby girl born in Richmond upon Thames is expected to live 17.8 more years in good health than a baby girl born in Manchester. Few would consider this just – there remains a lot of progress to achieve the society that Beveridge, the UN and Sen envisioned.
Box 3: Health as a human right in Scotland
Scotland’s National Action Plan for Human Rights encourages and coordinates efforts across government, local authorities, services, voluntary organisations and businesses to focus more on their human rights responsibilities in everything they do. These responsibilities include improving people’s health and wellbeing.
It was launched in 2013 and is a collaboration between the public and voluntary sectors, drawing on experiences around the world, as well as guidance from the United Nations and the Council of Europe.
Find out more: https://beta.gov.scot/policies/human-rights
The social case
Good health is an important enabler of positive family and community life. It enables people to participate in, and contribute to, society in different ways.
- A family member in good health is better able to build foundations that support other family members to thrive. For example, a parent providing emotional support for a child. On the other hand, health challenges such as childhood obesity and poor mental health can negatively affect family life and people’s ability to form and maintain good quality relationships.,,
- Having good health enables people to take part in civic society, including clubs and social groups, while poor health may hinder participation. In turn, engagement with communities can have a positive effect on social cohesion.
The economic case
Where a person stands in the labour market – such as whether they have a job that pays enough to live on – is key to their financial security and wellbeing.
Yet that person’s wellbeing throughout their life is also crucial to employers, businesses and the economy as a whole.
The potential economic benefits of ensuring the best possible health of the population are huge. A healthy population can be good for the economy because:
- healthier children have better educational outcomes, which positively impact productivity in adulthood,
- a healthy working-age population can lead to economic prosperity by being more engaged and productive
- a healthy person is enabled to continue to work as they get older, whereas poor health can lead to forced early retirement.,,,,
Conversely, a working-age population that is unwell, particularly with mental health problems, will likely negatively impact the UK economy.
- People with health problems are more susceptible to unemployment, lower earnings, sickness absence and lower household income.,,
- Every year, 300,000 people stop work and become reliant on health-related benefits.
- A further 140 million working days are lost to sickness, costing the UK economy £15bn.
Because poor work conditions can in turn affect health, a vicious cycle of poor health and poor wealth emerges, at huge cost to individuals, society and the economy.
A healthy population is therefore essential for a thriving society and economy.
We have a collective responsibility – to bring about a more stable and more prosperous world, a world in which every person in every country can reach their full potential.
Christine Lagarde, Managing Director, International Monetary Fund
Box 4: The value of health – research by the Health Foundation
Through the Health Foundation’s Social and Economic Value of Health research programme, we are building on the existing evidence for the role of good health as an asset for society and the economy.
This research forms part of a broader programme of work through which we aim to make the case that governments at all levels need to consider investment in maintaining and improving people’s health as synonymous with investing in the economy and society as a whole.
Find out more: www.health.org.uk/collection/socio-and-economic-value-good-health
What influences health and what can bring about change?
Estimates vary, but it is widely accepted that a population’s health is largely shaped by factors beyond access to health care.,, Rather than being something people just get at the doctor’s or at hospital, health is something that starts in families, schools, communities and workplaces. It can be found in parks and in the air people breathe.
The other factors that influence health – the social determinants – affect people in different ways, according to factors like age, gender, ethnicity, sexuality and disability. And they don’t operate in isolation. Rather, they are intricately woven together in a dynamic and mutually reinforcing way.
Take, for example, someone who doesn’t have the opportunity to do well at school. They are less likely to have a job and more likely to suffer poor health outcomes when they’re older.
However, the reason that person doesn’t do well at school might be that their home environment leads them to miss school, and the reason they will struggle to get a job may be partly due to high levels of unemployment in their community, or a lack of public transport to get to where the jobs are. Such factors are multiple and complex (see Figure 1).
Although some diseases are due to genetics, these play a much smaller role in shaping a person’s health than where they are born, grow, live, work and age.
It’s not your genetic code, it’s your [post]code.
Larry Cohen, Building a thriving nation
This can be illustrated by the underlying causes of obesity, which include advertising of unhealthy food and drink; workplaces and routines that restrict people being active; public spaces with few parks; and neighbourhoods where it’s difficult to buy affordable, healthy food.
Figure 1: The factors that influence an individual’s health and wellbeing
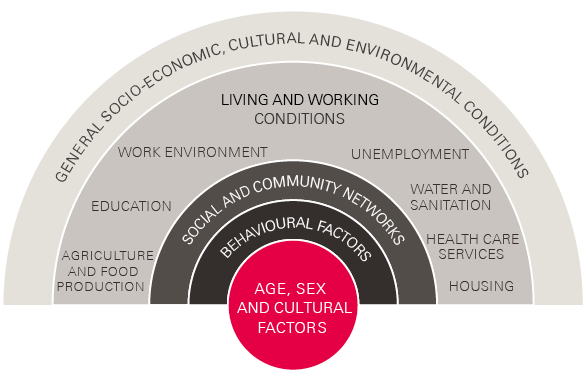
Source: Dahlgren and Whitehead.
These causes of the causes can influence our health and wellbeing in many ways, including through people’s health behaviours. Yet individual control over such behaviours is often very limited.
Unhealthy behaviours are usually not the origin of poor health, but the end point of a long chain of causes and consequences in people’s lives.
The rest of this section gives an overview of eight key social determinants of health (see Figure 2). The list is not definitive, but explains some of the key factors
in people’s physical and social environment that can be acted on to increase people’s opportunities to make healthy choices and to live healthy lives.
To show how different sectors might take action on the social determinants of health, we have included case studies to illustrate some direct and indirect ways change can happen.
The fact is that the conditions to which we are exposed influence our behaviour. Most of us cherish the notion of free choice, but our choices are constrained by the conditions in which we are born, grow, live, work and age.
Michael Marmot, The health gap
Figure 2: What makes us healthy?
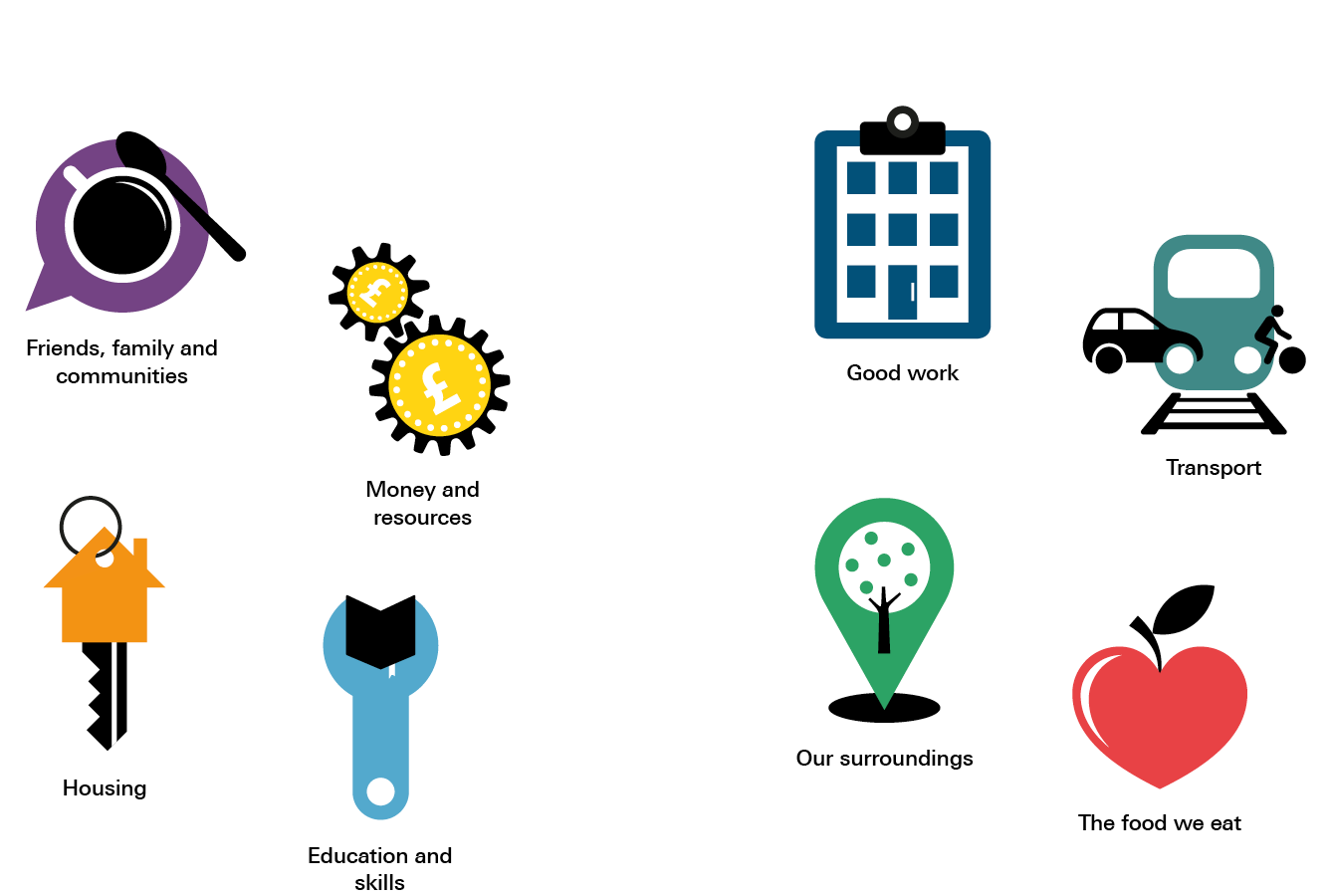
These images are based on an infographic series on the social determinants of health. Find out more: www.health.org.uk/healthy-lives-infographics
Family, friends and communities
Social isolation and loneliness are associated with a 30% increased risk of heart disease and stroke.
People who are more socially connected to family, friends or their community are happier and live longer, healthier lives with fewer physical and mental health problems than people who are less well connected.,
A positive family life provides a child with opportunities for a healthy life by creating the early life foundations for them to feel loved and valued; build supportive relationships; develop intellectual, social and emotional skills; and develop lifelong healthy habits. During adulthood, a positive family life, including strong spousal relationships, can have positive impacts on a person’s health and provide them with support to deal with life’s challenges.
Happy and positive friendships and feeling part of community life protects them from the damaging health effects of social isolation and provides them with opportunities to develop healthy habits. On the other hand, being lonely can have the opposite effect, such as by reducing the likelihood of exercise. Taking part in community life – such as youth clubs – can be empowering and create a sense of purpose, while also protecting health and wellbeing.
If we can create a society that brings people together, rather than isolating them, then we will not only have a happier society but one with less health costs to meet.
Dan Corry, New Philanthropy Capital
Case study 1: Men in Sheds – Age UK, Cheshire
In an industrial unit in Ellesmere Port, the Wirral, a group of men cluster around a lathe, listening carefully to the trainer. This is one of more than 400 Men in Sheds projects around the UK, targeting health and wellbeing in men aged over 50. The sheds act as a community hub, offering a host of activities, including woodwork and metalwork, plus space for a cup of tea.
For men, retirement or redundancy can lead to social isolation, especially for those who are single or widowed, but many are reluctant to seek help. The sheds provide an environment where men feel comfortable developing friendships and accessing support.
The sheds run social events and excursions and the men raise funds themselves, by selling the items they make. They also collaborate with local community groups and churches, including by building facilities for local schools.
Since the Ellesmere Port shed opened in 2008, the idea has taken off around the UK and beyond, with more than 2,000 shed projects worldwide. The model is evolving over time; for example, some now offer gyms and IT skills.
Find out more https://menssheds.org.uk
Money and resources
One in five people in the UK live in poverty, and over half of these people live in working households.
An inadequate income can cause poor health because it is more difficult to avoid stress and feel in control; access experiences and material resources; adopt and maintain healthy behaviours; and feel supported by a financial safety net.
Living with the day-to-day stresses of poverty in early childhood can have damaging consequences for long-term health. Money can enable people to access the support and services they need to participate fully in society. Yet, 48% of 21 to 24-year-olds earn less than the independently set living wage. An inadequate income can also make healthy behaviours feel unattainable: it is three times more expensive to get the energy we need from healthy foods than unhealthy foods.
Saving our planet, lifting people out of poverty, advancing economic growth... these are one and the same fight.
Ban Ki-moon, Secretary-General of the United Nations
A financial safety net enables people to invest in their future. In studies, 40% of people with unmanageable debt said they were less likely to study or retrain. Poverty damages health and poor health increases the risk of poverty.
Case study 2: Helping wealth stay local – Preston City Council
Since 2011, Preston has been exploring alternative approaches to local economic development that also reduce inequality. One scheme is the Community Wealth Building initiative, which involved cooperating with six local organisations known as ‘anchor institutions’.
The combined procurement spend of these institutions (one of which was Preston City Council) was £750m in 2012/13, but only 5% of this was spent in Preston. The institutions committed to diverting more spend to local businesses.
The scheme included the city’s key employers: the hospital, a housing association and the university. Local suppliers received advice on how to pitch for contracts, which included a £60,000 printing contract for the police and a £1.6m contract to provide school meals, which was divided into lots and awarded to suppliers who use local farmers.
The benefits of this approach are already visible. The six anchor institutions increased their spending with Preston-based suppliers from 5% of total spend in 2012 to 18% in 2017 – an increase of £74m. It is estimated this increase supports around 1,648 local jobs. The city has also made improvements on six out of eight of its local authority summary deprivation measures between 2010 and 2015.
Find out more: https://cles.org.uk/publications/community-wealth-building-through-anchor-institutions
Housing
Children living in cold homes are more than twice as likely to suffer from respiratory problems than children living in warm homes.
Where people live is more than just a roof over their heads. It’s their home, where they grow up and flourish. A healthy home is affordable, warm and stable: somewhere safe that meets the diverse needs of the people living there and helps them connect to community, work and services.
Investing in housing support for vulnerable people helps keep them healthy. Every £1 invested delivers nearly £2 of benefit through costs avoided to public services including care, health and crime costs.
A safe settled home is the cornerstone on which individuals and families build a better quality of life, access services they need and gain greater independence.
Jake Eliot, Head of Policy, Money Advice Service
Case study 3: Linking fuel poverty to health outcomes – Warm Homes Nest Scheme, Wales
Poor housing stock and mainly rural communities mean that fuel poverty has been a major problem in Wales. To tackle the issue, the government set up the Warm Homes Nest Scheme to target households with the greatest need.
To evaluate the project, the government has linked anonymised data from the scheme with routine health records. This allows the evaluators to analyse the impact of the scheme on individual health. The results have been impressive, with evidence of positive effects on people’s health.
Over the course of a year, for households who received help with their energy efficiency, the average number of times a person had to go to a GP for breathing problems decreased by 3.9% for those on the scheme, and they also experienced a 6.5% decrease in asthma events. These factors increased among people who were eligible for, but not on, the scheme.
Find out more: www.nestwales.org.uk
Education and skills
People with the lowest healthy life expectancy are three times more likely to have no qualifications compared with those with the highest life expectancy.
Good education and skills can help build strong foundations for supportive social connections, accessing good work, lifelong learning and problem solving, and feeling empowered and valued.
These help people live healthier lives by increasing their opportunities to develop lifelong healthy habits; afford a good quality of life; live and work in safe and healthy environments; and manage and limit exposure to life’s challenges.
The prize [of good education] is simple: healthier, happier, wealthier people, and stronger families, communities and businesses.
David Hughes, Chief Executive, Association of Colleges
Case study 4: Boosting employability in young people – The North East Ambition programme
The opportunities available to young people on leaving school are pivotal to their futures. Young people who are not in education, employment or training are more likely to suffer worse health outcomes in later life, so targeting this group is an important priority for society.
In 2015, the north east had the highest rate of young people who are not in education, employment or training in the country, so the North East Local Enterprise Partnership started intensive work to tackle this issue. One aim of the programme was for 170 local secondary schools and colleges in the area to meet the eight Good Career Guidance Benchmarks.
These include personal guidance tailored to each pupil, work experience and encounters with employers. The programme was supported by several new cross-sector networks bringing schools, colleges and businesses together to share ideas and pool resources.
2 years after the programme’s launch, 85% of the 70 participating schools and colleges had reached six or more of the Good Career Guidance Benchmarks. Partly as a result of this work, the rate of young people not in education, employment or training in the north east has dropped from 23.4% to 13.5%. The benchmarks have also been adopted as part of the Department for Education’s national career strategy.
Find out more: www.nelep.co.uk/skills/north-east-ambition
Good work
Young adults who are unemployed are more than twice as likely to suffer from mental ill health than those in work.
Good work offers stability, security and a regular income. It provides good working conditions, including a safe working environment, good wages and practices that protect employees’ wellbeing. It provides an environment in which employees are supported, have personal development opportunities, and a degree of control and autonomy over their work.
Ultimately, gaining or maintaining ‘good’ employment and improving workplace health has the potential to make a significant contribution to personal wellbeing, the economy and reducing levels of disease and illness in society.
Good work provides opportunities to afford basic living standards; participate in community and social life; support lifelong healthy habits; and feel a sense of identity, self-esteem, purpose and reward. It offers protection against the harmful effects of unemployment and insecure jobs, which can damage long-term health and wellbeing.
Case study 5: Incentivising employers to boost staff mental health – Thrive West Midlands
There are an estimated 70,000 people in the West Midlands who are out of work as a result of mental health problems. The West Midlands Combined Authority’s Mental Health Commission launched an action plan to address the wide impact this has on the region – not least on the local economy, as well as individuals and communities.
A core part of the plan is the workplace wellbeing premium, which will provide a financial incentive for employers to introduce measures that support the mental health and wellbeing of their workforce. This pilot scheme provides organisations with a grant and various toolkits and resources. These are intended to help them capture and use data better, and put in place initiatives to promote a culture of wellbeing.
The scheme is supported by more than 120 signatories, including the police, local authorities, schools and housing associations, and has been developed with support from people with mental health problems.
Find out more: www.wmca.org.uk/media/1420/wmca-mental-health-commission-thrive-full-doc.pdf
Transport
There are nine times as many fatal and serious injuries among pedestrians aged 5–9 in the most deprived areas than the least.
Healthy transport systems support safe and well-designed communities. They enable more walking, cycling and public transport use, are accessible and efficient for everyone, and minimise harmful impacts of the environment. This helps people to lead healthier lives. For example, people who use public transport are likely to do an extra 12–15 minutes physical activity each day.
Streets and public spaces that are well designed also encourage active travel, and can have other positive impacts such as reducing vehicle speeds.
Transport is not an end in itself, but rather a means... to access what [people] need: jobs, markets and goods, social interaction, education, and a full range of other services contributing to healthy and fulfilled lives.
United Nations Secretary-General’s High-Level Advisory Group on Sustainable Transport
A healthy transport system can provide opportunities to improve air quality – the largest contributor to air pollution in London is road transport. It can also help hard-to-reach or deprived communities to access key services, such as learning opportunities and jobs.
Case study 6: Reducing inequalities through transport – Manchester Metrolink
The Manchester Metrolink is the largest light rail system in the UK. Its benefits to the community have reached beyond transport links, thanks to the vision of local transport planners.
Transport for Greater Manchester collaborated with local authorities to improve connections for 2.7 million residents. Its contribution, along with other public and private sector collaboration, focused on a common goal and long-term economic vision: to use transport to connect commuters from around Greater Manchester to key industrial and commercial districts.
As a result, the system is having a positive influence on the social determinants of health. The latest extension to Oldham and Rochdale town centres, East Didsbury and Ashton-under-Lyne has improved access to employment for 16 to 70-year-olds, further education options for 16 to 19-year-olds, and health care for the whole population. Improved accessibility to these services through public transport has been more marked for the 10% most deprived areas along this route, helping to reduce inequalities.
Find out more: www.volkerrail.co.uk/dynamics/modules/SFIL0200/view.php?fil_Id=8932
Our surroundings
Children in deprived areas are nine times less likely to have access to green space and places to play.
Health is influenced by how surroundings make people feel and the opportunities they provide. Good places, spaces and buildings enable people to be more physically active, feel safe and secure, use facilities and services, and socialise and play. For example, well maintained and easy to reach green space makes it easier for people to be physically active.,
Being near facilities and services like shops and schools makes it easier to walk to them – this can, for example, help reduce social isolation among older people.
It turns out that the key elements necessary for public space to improve people’s health are the same as those needed to make urban space socially and economically vibrant and environmentally sustainable.
Lucy Saunders, Public Health Specialist, Transport for London
Case study 7: Investing in healthy streets – Greater London Authority
Recognising the relationship between transport and health, in 2014 Transport for London became the first transport authority in the world to publish a Health Action Plan. It has adopted the Healthy Streets approach, which will help it improve air quality, reduce congestion and create healthy surroundings for people to live, work, commute and play.
The Healthy Streets approach is based on 10 evidence-based indicators. The approach defines a healthy street as one with: things to see and do; places to stop and rest; shade and shelter; clean air; and pedestrians from all walks of life. It must also be easy to cross; and feel safe, relaxing and not too noisy. Put simply, it needs to be an environment in which people choose to walk and cycle.
Action against these indicators ultimately improves health. Transport for London has committed to delivering improvements against these indicators through the 25-year Mayor’s Transport Strategy.
This approach was applied in Archway in north London, which was a large traffic-dominated gyratory. Through a transformative project the 10 indicators showed an overall uplift. Importantly, seven road danger issues were eliminated through the redesign of the junction.
Find out more https://tfl.gov.uk/corporate/about-tfl/how-we-work/planning-for-the-future/healthy-streets
The food we eat
It is three times more expensive to get the energy we need from healthy food than unhealthy food.
Poor diet is the one of the biggest risk factors for preventable ill health in England. Everyone should have enough good food to live a healthy life. Healthy food needs to be: affordable for everyone, a bigger part of the food supply chain, available in local areas, and promoted and valued.
Yet many factors in our environment make it hard to eat healthily. It is harder to buy healthy foods in deprived parts of the UK. There is also a higher density of fast food outlets in these areas. The promotion of food may also make healthy behaviours harder: just 1.2% of advertising spend each year goes on vegetables, compared with the 22% spent on confectionary, cakes, biscuits and ice cream.
The healthy choice should be the easy choice.
Rob Beaglehole, Public Health Dentist
Case study 8: Using planning to restrict takeaways – Gateshead Council
Access to healthy food goes far beyond the control of an individual. With this in mind, Gateshead Council has used local planning policy to improve the opportunities its residents have to make healthy food choices. The ambition is to reduce levels of obesity and, in turn, deaths from cancers and circulatory diseases. The approach focuses on reducing health inequalities in Gateshead.
The council won a Local Communities and Government award for its innovative approach: developing a supplementary planning document under its local plan.
This new document means that any application for a hot food takeaway will be declined if it is in an area where more than 10% of children in year 6 are obese; if it is within 400m of secondary schools and other community amenities, or if the number of hot food takeaways in the area is equal to or greater than the UK national average.
The award was made in recognition of the strong joint working between the local elected members, planning teams and public health teams. Judges said the council deserved to win because it had used ‘a strategic, holistic approach with strong political buy-in to tackle a major public health issue, making best use of local authority mechanisms.’
‡ For the full list of benchmarks developed by Gatsby see: www.gatsby.org.uk/education/focus-areas/good-career-guidance
§ Nearly 75% of people who are in the bottom fifth of income distribution and rent privately pay more than a third of their income in rent.
¶ Healthy Streets is an evidence-based approach for creating sustainable, attractive urban spaces. Find out more: https://healthystreets.com
Fair opportunities for healthy lives
Everyone in society should have the opportunity to make healthy choices and live healthy lives. But inequalities in power, money and resources at local, national and even global levels can make the circumstances of people’s daily lives more challenging. In turn, such circumstances can make people more vulnerable to poor health.
Although people are now living longer than they used to, the fact remains that socially disadvantaged people are more likely to face conditions – such as insecure work, or living in a run-down neighbourhood – that lead to poorer health and an earlier death.
These differences in people’s health and wellbeing are called health inequalities, and they don’t just exist between the very rich and the very poor in society: they span the population and affect people of all ages, at every stage of life, and across all major diseases.
Like slavery and apartheid, poverty is not natural. It is man-made and can be overcome and eradicated by the actions of human beings.
Nelson Mandela, former President of South Africa
It is possible to provide opportunities for people to live healthy lives. Decision makers at all levels can create policies – from international trade deals to lowering local levels of congestion – that will enable people to have greater influence over their own health and health behaviours, as well as those of their families.
The action required is universal: focusing solely on the most disadvantaged would only tackle part of the problem. If action is proportionate to the level of disadvantage, there is an opportunity to both improve the health of the population and reduce health inequalities.
The Marmot review, Fair society, healthy lives, concluded that reducing health inequalities in the UK requires a series of objectives to be met. These are:
- giving every child the best possible start in life
- creating job opportunities and fair working conditions for all
- ensuring a healthy standard of living for the whole population
- developing health-creating physical environments
- empowering communities
- strengthening health prevention.
** Alongside these policy objectives are a set of indicators developed to help people monitor change at local and national level. Find out more: https://fingertips.phe.org.uk/profile/wider-determinants
Who can influence the social determinants of health?
At the beginning of this guide, we talked about heart disease and its root causes. By taking action to address these root causes it is possible to prevent many people having heart attacks.
Changing and improving local environments is a more just and effective way to influence the health and wellbeing of an entire population than waiting for people to become ill and treating them as patients, one person at a time.
Yet there is no single idea or policy that will improve the health of the public. Solutions require all members of society to acknowledge the health impact of what they do and work together to take action. If this happens, we could see improvements in people’s health and a reduction in the health inequalities that exist between different groups in society.
The case studies in Section 4 show how efforts to impact the social determinants of health are taking place across a range of sectors. These efforts involve community empowerment, partnership working, helping those most in need, and incorporating health and wellbeing in all policy decisions (reaching far beyond the Department of Health itself). Such action protects people’s health and helps to provide environments that create health and wellbeing. It also highlights the potential that everyone in society has to improve people’s health, either by directly focusing on the social determinants or explicitly addressing health in everything they do.
Change is never easy – especially in changing political and financial contexts. Often, decisions involve difficult trade-offs. Sometimes, the benefits of action taken in one sector are reaped by another. Nevertheless, organisations are finding ways to come together to tackle the social determinants of health, and must continue to do so.
The single most important intervention is to understand that there is no single most important intervention.
Harry Rutter, London School of Hygiene and Tropical Medicine
What can I do to make a difference?
It can be hard to know where to start, but even small changes can influence thinking, narrative and policy. It is likely that such changes would make a difference to people’s health.
Considering the social determinants of health we have outlined in this guide, do you think the last decision you took (or the next one you take) might:
- have an impact on one or more of the social determinants?
- have an impact on health and wellbeing?
- increase or decrease health inequalities?
If the answer is yes to any of those questions, we would ask you to consider:
- how, in the work you’re already doing, you could more explicitly address health and wellbeing
- approaching others to discuss joint working initiatives in new areas where both parties benefit
- talking to your local public health team or a public health expert to find out more about what you can do
- using the facts, figures and case studies in this guide in presentations, reports or funding bids
- engaging others about the part they already play in improving people’s health.
Further resources
What is already happening?
The following section provides more examples of where change is already taking place. The initiatives listed here span efforts across national and local government – as well as the private and voluntary sectors.
National government
|
The Wellbeing of Future Generations (Wales) Act 2015: An act that makes health a prerequisite for all policy. Proposals must demonstrate tangible benefits for the health and wellbeing of current and future generations. This integrated approach will maximise health promotion and increase understanding among the public that health is influenced by multiple determinants in different sectors. Find out more: http://thewaleswewant.co.uk/sites/default/files/150623-guide-to-the-fg-act-en.pdf |
|
Minimum unit price for alcohol (Scotland) 2018: Legislation for a minimum unit price for alcohol, to help cut alcohol-related deaths and reduce hospital admissions. Find out more: www.legislation.gov.uk/asp/2012/4/contents/enacted |
|
Soft drinks industry levy (UK) 2018: A levy to target the producers and importers of soft drinks with added sugar, to help protect people from tooth decay, obesity and diabetes. Find out more: www.gov.uk/guidance/soft-drinks-industry-levy |
|
The Smoking (Northern Ireland) Order 2006: Smoke-free legislation that makes it illegal to smoke in workplaces, on public transport and in many enclosed public spaces. Find out more: www.legislation.gov.uk/nisi/2006/2957/contents |
Local government
|
Coventry City Council: A council that has partnered with Public Health England and the Institute of Health Equity to work together as a ‘Marmot City’ and reduce inequalities in Coventry. This involves taking action on the social determinants of health and ensuring health, social value and asset-based approaches are reflected in everything the council does. Find out more: www.coventry.gov.uk/downloads/download/4171/coventry_a_marmot_city |
|
Wigan Council: A council that is thinking outside the box to engage residents and community groups through an informal agreement between the council and the people who live and work there. Through this agreement – known as The Deal – it is co-designing public services to make Wigan a better place to live. Find out more: www.wigan.gov.uk/Docs/PDF/Council/The-Deal/The-Deal-Brochure.pdf |
Voluntary sector
|
Shelter: Alongside charities like the Health Foundation, non-health charities and those that aren’t pursuing a health-focused mission are still helping to support and improve people’s health. Shelter helps millions of people every year who are struggling with poor housing and homelessness, and monitors health outcomes of its clients. |
|
Citizen’s Advice: A charity that provides holistic and tailored support, helping people with a range of problems such as managing debt, or dealing with housing and employment issues. Citizen’s Advice has used a New Economy Tool to estimate the impact of its work on health. |
|
Find out more about how non-health charities can address the social determinants of health: |
Communities
|
Bromley by Bow Health Partnership: An innovative community organisation in east London, working in one of the most deprived boroughs in the UK. It supports families, young people and adults to learn new skills, improve their health and wellbeing, find employment and develop confidence to achieve their goals. The partnership is considered a flagship example of community led regeneration. Find out more: www.bbbhp.co.uk |
Funders
|
People’s Health Trust: Invests in resident-led approaches to address underlying structural causes of health inequalities. Its long-term engagement programme, Local Conversations, makes the most of local residents’ skills and wisdom by putting them in control of the design, development and action in their neighbourhood. Find out more: www.peopleshealthtrust.org.uk |
|
Big Lottery Fund: A funder that gives grants to organisations in the UK to help improve their communities. Find out more: www.biglotteryfund.org.uk |
Businesses and employers
|
Timpsons: A company that employs ex-offenders and those from marginalised groups. It provides good pay and flexible working conditions related to work hours, childcare, sabbaticals and study leave, to support the physical and mental wellbeing of those who face significant barriers to the workplace. Find out more: www.timpson.co.uk/about/careers-at-timpson |
|
Business and Sustainable Development Commission: An organisation that aims to mobilise a community of businesses to take action on the UN’s sustainable development goals and achieve greater social and environmental sustainability. Find out more: http://businesscommission.org |
Where can I find out more?
The following are a selection of key organisations that provide further information and case studies on the social determinants of health.
|
Glasgow Centre for Population Health |
|
Institute of Health Equity |
|
Joseph Rowntree Foundation |
|
Local Government Association www.local.gov.uk/topics/social-care-health-and-integration/public-health |
|
NHS Health Scotland |
|
Public Health Agency (Northern Ireland) |
|
Public Health England |
|
Public Health Wales Observatory |
|
Robert Wood Johnson Foundation |
|
Royal Society for Public Health |
|
The King’s Fund |
|
What Works Centre for Wellbeing |
|
World Health Organization |
|
See also the Health Foundation’s compendium of resources and case studies: |
References
- National Institute for Health and Care Excellence. Health inequalities and population health. 2012. Available from: www.nice.org.uk/advice/lgb4/resources/health-inequalities-and-population-health-1681147764421
- Aboriginal Health and Medical Research Council of New South Wales. Definition of Aboriginal Health. Available from: www.ahmrc.org.au/index.php?option=com_content&view=article&id=35&itemid=37
- What Works Centre for Wellbeing. Available from: www.whatworkswellbeing.org
- Stuckler D. The Body Economic: Why Austerity Kills. Basic Books; 2013.
- World Health Organization. Constitution of the World Health Organization. 2006. Available from: www.who.int/about/mission
- Sen A. Commodities and Capabilities. North-Holland; 1985.
- Office for National Statistics. Statistical bulletin: healthy life expectancy at birth and aged 65 by upper tier local authority and area deprivation: England 2012–14. 2016.
- Waylen A, Stewart-Brown S. Factors influencing parenting in early childhood: a prospective longitudinal study focusing on change. Child: Care, Health and Development. 2010;36(2):198–207.
- Griffiths LJ, Dezateux C, Hill A. Is obesity associated with emotional and behavioural problems in children? Findings from the Millennium Cohort Study. Int J Pediatr Obes. 2011;6(2-2):E423–E32 a.
- Clarke H, McKay S. Disability, partnership and parenting. Disability & Society. 2014;29(4):543–55.
- Colman I et al. Outcomes of conduct problems in adolescence: 40 year follow-up of national cohort. BMJ. 2009;338:a2981.
- Matthews K, Nazroo J, Whillans J. The consequences of self-reported vision change in later-life: evidence from the English Longitudinal Study of Ageing. Public Health. 2017;142:7–14.
- Jivraj S, Nazroo J, Barnes M. Short- and long-term determinants of social detachment in later life. Ageing & Society. 2016;36(5):924–45.
- Yamey G et al. Investing in health: the economic case. World Innovation Summit for Health; 2016. Available from: http://globalhealth2035.org/sites/default/files/investing-in-health-economic-case.pdf
- Case A, Fertig A, Paxson C. The lasting impact of childhood health and circumstance. Journal of Health Economics. 2005;24(2):365–89.
- Disney R, Emmerson C, Wakefield M. Ill health and retirement in Britain: a panel data-based analysis. Journal of Health Economics. 2006;25(4):621–49.
- Jones AM, Rice N, Roberts J. Sick of work or too sick to work? Evidence on self-reported health shocks and early retirement from the BHPS. Economic Modelling. 2010;27(4):866–80.
- Stafford M et al. Physical and cognitive capability in mid-adulthood as determinants of retirement and extended working life in a British cohort study. Scand J Work Environ Health. 2017;43(1):15–23.
- Rice NE et al. Common health predictors of early retirement: findings from the English Longitudinal Study of Ageing. Age and Ageing. 2011;40(1):54–61.
- Rumball-Smith J et al. Diabetes associated with early labor-force exit: a comparison of sixteen high-income countries. Health Affairs. 2014;33(1):110-5.
- Henderson M et al. A lifecourse approach to long-term sickness absence – a cohort study. PLOS One. 2012;7(5):e36645.
- Stansfeld SA et al. Psychosocial work characteristics and anxiety and depressive disorders in midlife: the effects of prior psychological distress. Occup Environ Med. 2008;65(9):634–42.
- Johnston DW, Schurer S, Shields MA. Exploring the intergenerational persistence of mental health: evidence from three generations. Journal of Health Economics. 2013;32(6):1077–89.
- Black C, Frost D. Health at work – an independent review of sickness absence. 2011. Available from: www.gov.uk/government/uploads/system/uploads/attachment_data/file/181060/health-at-work.pdf
- Lagarde C. An address to the 2011 International Finance Forum. 9 November 2011. Available from: www.imf.org/en/News/Articles/2015/09/28/04/53/sp110911
- McGovern L, Miller G, Hughes-Cromwick P. Health Policy Brief: The relative contribution of multiple determinants to health outcomes. Health Affairs. 21 August 2014.
- James C, Devaux M, Sassi F. Inclusive growth and health. OECD Publishing; 2017. Available from: http://dx.doi.org/10.1787/93d52bcd-en
- Robert Wood Johnson Foundation. A new way to talk about the social determinants of health. 2010. Available from: www.rwjf.org/content/dam/farm/reports/reports/2010/rwjf63023
- Marmot M. Fair society, healthy lives: The Marmot review. 2010. Available from: www.parliament.uk/documents/fair-society-healthy-lives-full-report.pdf
- Cohen L. Building a thriving nation: 21st century vision and practice to advance health and equity. Health Education & Behavior. 2016; 43(2):125–32.
- Whitehead M, Dahlgren G. What can be done about inequalities in health? The Lancet. 1991;26(338)8774:1059–1063.
- L’Hôte E, Fond M, Volmert A. Research into: Seeing upstream: Mapping the gaps between expert and public understandings of health in the United Kingdom. FrameWorks Institute (unpublished).
- Marmot M. The health gap: the challenge of an unequal world. Bloomsbury; 2015.
- Valtorta NK et al. Loneliness and social isolation as risk factors for coronary heart disease and stroke: systematic review and meta-analysis of longitudinal observational studies. Heart. 18 April 2016.
- Mental Health Foundation. Relationships in the 21st century: the forgotten foundation of mental health and wellbeing. 2016. Available from: www.mentalhealth.org.uk/publications/relationships-21st-century-forgotten-foundation-mental-health-and-wellbeing
- Berkman LF, Syme SL. Social networks, host resistance, and mortality: a nine-year follow-up study of Alameda County residents. Am J Epidemiol. 1979;109(2):186–204
- Allen M, Donkin A. The impact of adverse experiences in the home on the health of children and young people, and inequalities in prevalence and effects. UCL Institute of Health Equity; 2015. Available from: http://cdn.basw.co.uk/upload/basw_13257-1.pdf
- Dyson et al. Childhood development, education and health inequalities. Report of task group. Submission to the Marmot Review. Available from: www.ucl.ac.uk/gheg/marmotreview/consultationEarly_years_and_education_report
- Bellis et al. National household survey of adverse childhood experiences and their relationship with resilience to health-harming behaviors in England. BMC medicine. 2014;12:72
- Kiecolt-Glaser JK, Newton TL. Marriage and health: his and hers. Psychological Bulletin. 2001;127(4):472.
- Uchino BN, Cacioppo JT, Kiecolt-Glaser JK. The relationship between social support and physiological processes: a review with emphasis on underlying mechanisms and implications for health. Psychological Bulletin. 1996;119(3):488.
- Hawkley LC, Thisted RA, Cacioppo JT. Loneliness predicts reduced physical activity: Cross-sectional & longtitudinal Analyses. Health Psychology. 2009; 28(3):354–363.
- Daly S, Allen J. Inequalities in mental health, cognitive impairment and dementia amongst older people. UCL Institute of Health Equity; 2016. Available from: http://cdn.basw.co.uk/upload/basw_53658-8.pdf
- Handley S et al. The best medicine? The importance of relationships for health and wellbeing. Relate and New Philanthropy Capital; 2015. Available from: www.relate.org.uk/sites/default/files/publication-the-best-medicine-report-240315.pdf
- Joseph Rowntree Foundation Analysis Unit. UK Poverty 2017: a comprehensive analysis of poverty trends and figures. 2017. Available from: www.jrf.org.uk/report/uk-poverty-2017
- Fell B, Hewstone M. Psychological perspectives on poverty. Joseph Rowntree Foundation; 2015. Available from: www.jrf.org.uk/report/psychological-perspectives-poverty
- Office for National Statistics. Proportion of employees earning below £8.75 per hour working outside London, £10.20 per hour working in London: April 2017. 2017.
- Jones NRV et al. The growing price gap between more and less healthy foods: analysis of a novel longitudinal UK dataset. PLOS One. 2014;9(10):e109343.
- United Nations Foundation. Sustainable energy for all a priority for UN Secretary-General’s second term. Available from: www.unfoundation.org/news-and-media/press-releases/2011/energy-for-all-a-priority-for-un-secretary-general.html
- Lane J. A debt effect? How is unmanageable debt related to other problems in people’s lives? Citizens Advice; 2016. Available from: www.citizensadvice.org.uk/about-us/policy/policy-research-topics/debt-and-money-policy-research/a-debt-effect
- Benzeval M et al. How does money influence health? Joseph Rowntree Foundation; 2014. Available from: www.jrf.org.uk/report/how-does-money-influence-health
- Centre for Local Economic Strategies. Updating the spend analysis baseline: summary report. 2017. Available from: www.preston.gov.uk/thecouncil/about-preston-city-council/our-fairness-agenda/progress-towards-fairness-charter
- Preston City Council. Community Wealth Building. Co-operative Councils Innovation Network; 2017. Available from: www.councils.coop/wp-content/uploads/2017/10/Community-Wealth-Building-Preston-City-Council.pdf
- Lancashire County Council Business Intelligence Team. The English indices of deprivation 2015, local authority level analysis. Lancashire County Council; 2015. Available from: www.lancashire.gov.uk/media/898623/deprivation-2015-la-summaries.pdf
- Marmot Review Team (Geddes I, Bloomer E, Allen J, Goldblatt P). The health impacts of cold homes and fuel poverty. Friends of the Earth; 2011. Available from: https://friendsoftheearth.uk/sites/default/files/downloads/cold_homes_health.pdf
- Audit Commission. Building better lives: getting the best from strategic housing (local government). 2009. Available from: www.bl.uk/collection-items/building-better-lives-getting-the-best-from-strategic-housing-local-government
- de Sa J. Infographic: how does housing influence our health? Health Foundation; 2017. Available from: www.health.org.uk/blog/infographic-how-does-housing-influence-our-health
- Office for National Statistics. An overview of lifestyles and wider characteristics linked to Healthy Life Expectancy in England: June 2017. 2017.
- Egerter S et al. Exploring the social determinants of health: Education and health. Robert Wood Johnson Foundation; 2011. Available from: www.rwjf.org/content/dam/farm/reports/issue_briefs/2011/rwjf70447
- Hughes D. Teachers: the hidden public health workforce. Health Foundation; 2017. Available from: www.health.org.uk/blog/teachers-hidden-public-health-workforce
- Social Mobility Commission. State of the nation 2017: social mobility in Great Britain. 2017. Available from: www.gov.uk/government/uploads/system/uploads/attachment_data/file/662744/State_of_the_Nation_2017_-_Social_Mobility_in_Great_Britain.pdf
- UCL Institute of Education. Being on a zero-hours contract is bad for your health, new study reveals. 5 July 2017. Available from: www.ucl.ac.uk/ioe/news-events/news-pub/jul-2017/zero-hours-contract-bad-for-health
- Commission on Social Determinants of Health. Closing the gap in a generation: health equity through action on the social determinants of health. World Health Organization; 2008.
- The Health Foundation and the All-Party Parliamentary Health Group. A healthier life for all: the case for cross-government action. 2016. Available from: www.health.org.uk/publication/healthier-life-all
- Marmot M et al. Health inequalities among British civil servants: the Whitehall II study. The Lancet. 1991;337(8754):1387–1393.
- Stansfeld S, Candy B. Psychosocial work environment and mental health – a meta-analytic review. Scand J Work Environ Health. 2006;32(6):443–62.
- Kim TJ, von dem Knesebeck O. Is an insecure job better for health than having no job at all? A systematic review of studies investigating the health-related risks of both job insecurity and unemployment. BMC Public Health. 2015;15:985
- Public Health England. Reducing unintentional injuries on the roads among children and young people under 25 years. 2014. Available from: www.gov.uk/government/publications/reducing-unintentional-injuries-among-children-and-young-people
- Rissel C et al. Physical activity associated with public transport use – a review and modelling of potential benefits. Int J Env Res and Public Health. 2012;9(7):2454–78.
- Woolley H et al. The value of public space: how high quality parks and public spaces create economic, social and environmental value. CABE Space. Available from: www.designcouncil.org.uk/sites/default/files/asset/document/the-value-of-public-space1.pdf
- United Nations Secretary-General’s High-Level Advisory Group on Sustainable Transport. Mobilizing sustainable transport for development. 2016. Available from: https://sustainabledevelopment.un.org/content/documents/2375Mobilizing%20Sustainable%20Transport.pdf
- Institute of Public Policy Research. Lethal and illegal. Solving London’s air pollution crisis. Available from: www.ippr.org/files/publications/pdf/lethal-and-illegal-solving-londons-air-pollution-crisis-Nov2016.pdf
- National Children’s Bureau. Greater Expectations: raising aspirations for our children. 2013. Available from: www.ncb.org.uk/sites/default/files/uploads/documents/Policy_docs/GEXP_final%20WEB.pdf
- NHS Health Scotland. Place and communities. 2016. Available from: www.healthscotland.scot/media/1088/27414-place-and-communties-06-16.pdf
- Balfour R, Allen J. Local action on health inequalities: improving access to green spaces. Public Health England and UCL Institute of Health Equity; 2014. Available from: www.gov.uk/government/publications/local-action-on-health-inequalities-evidence-papers
- Public Health England. Spatial Planning for health: an evidence resource for planning and designing healthier places. 2017. Available from: www.gov.uk/government/uploads/system/uploads/attachment_data/file/625568/Spatial_planning_for_health_an_evidence_resource.pdf
- Healthy Streets. Available from: https://healthystreets.com
- Williamsomn et al. Deprivation and healthy food access, cost and availability: a cross-sectional study. Human Nutrition and Dietics. 2017:30(6)
- Public Health England. Obesity and the environment: density of fast food outlets. 2016. Available from: www.gov.uk/government/uploads/system/uploads/attachment_data/file/578041/Fast_food_map_2016.pdf
- Nielsen AdDynamix. Cited in: Food Foundation. Veg Facts. 2016. Available from: http://foodfoundation.org.uk/wp-content/uploads/2016/11/FF-Veg-Doc-V5.pdf
- Eder J. New Zealand dentist Rob Beaglehole convinces World Health Organisation to remove sugary drinks. Stuff; 23 November 2016. Available from: www.stuff.co.nz/national/health/86717246/new-zealand-dentist-rob-beaglehole-convinces-world-health-organisation-to-remove-sugary-drinks
- Mandela N. In full: Mandela’s poverty speech. BBC; February 2005. Available from: http://news.bbc.co.uk/1/hi/uk_politics/4232603.stm
- Rutter H. The single most important intervention to tackle obesity… Int J Public Health. 2012;57(4)657–8.